OUR LADY SEAT OF WISDOM UMBRELLA TRUST - Managing Medicines in School
![]()
Company number 8180450
This school is committed to reducing the barriers to sharing in school/nursery life and learning for all its pupils. This policy sets out the steps which our school will take to ensure full access to learning for all its children who have medical needs and are able to attend school.
N.B Paragraph numbers refer to the DfE publication Managing Medicines in Schools and Early Years Settings.
1. Managing prescription medicines which need to be taken during the school day.
1.1 Parents/carers should provide full written information about their child’s medical needs.
1.2 Short-term prescription requirements should only be brought into school if it is detrimental to the child’s health not to have medicine during the school day. If the period of administering medicine is 8 days or more, there must be an Individual Health Care Plan. Paragraph 37
1.3 The school will not accept medicines that have been taken out of the container as originally dispensed nor will it make changes to prescribed dosage. Paragraph 26
1.4 The school will not administer medicines that have not been prescribed by a doctor, dentist, nurse prescriber or pharmacy prescriber, unless it is done as part of an individual health care plan. The school will inform parents of this policy. Paragraph 25
1.5 Some medicines prescribed for children (e.g. methylphenidate, known as Ritalin) are controlled by the Misuse of Drugs Act. Members of staff are authorised to administer a controlled drug, in accordance with the prescriber’s instructions. A child may legally have prescribed controlled drugs in their possession. The school will keep controlled drugs in a lockable non portable container, to which named staff will have access. A record of access to the container will be kept. Misuse of a controlled drug is an offence, and will be dealt with under the school’s behaviour policy.
1.6 Medicines should always be provided in the original container as dispensed by a pharmacist and should include the prescribers instructions for administration. In all cases this should include:
- Name of child
- Name of medicine
- Dose
- Method of administration
- Time/ frequency of administration
- Any side effects
- Expiry date
1.7 The school will refer to the DfE guidance document when dealing with any other particular issue relating to managing medicines.
2. Procedures for managing prescription medicines on trips and outings and during sporting activities
2.1 The school will consider what reasonable adjustments might be made to enable children with medical needs to participate fully and safely on visits. This may extend to reviewing and revising the visits policy and procedures so that planning arrangements incorporate the necessary steps to include children with medical needs. It might also incorporate risk assessments for such children. Paragraph 56
2.2 If staff are concerned about how they can best provide for a child’s safety, or the safety of other children on a visit, they should seek parental views and medical advice from the school health service or the child’s GP. Please refer to the DfE guidance on planning educational visits. Paragraph 58
2.3 The School will support children wherever possible in participating in physical activities and extra-curricular sport. Any restriction on a child’s ability to participate in PE should be recorded on their Health Care Plan. Paragraph 60
2.4 Some children may need to take precautionary measures before or during exercise, and may need access, for example, to asthma inhalers. Staff supervising sporting activities will be made aware of relevant medical conditions, and will consider the need for a risk assessment to be made. Paragraph 61
2.5 The school must cooperate with the Local Authority in fulfilling its responsibilities regarding home to school transport. This may include giving advice regarding a child’s medical needs.
3. The roles and responsibilities of staff managing administration of medicines, and for administering or supervising the administration of medicines
3.1 Close co-operation between school, settings, parents/carers, health professionals and other agencies will help provide a suitably supportive environment for children with medical needs.
3.2 It is important that responsibility for child safety is clearly defined and that each person responsible for a child with medical needs is aware of what is expected of them.
3.3 The school will always take full account of temporary, supply and peripatetic staff when informing staff of arrangements for the administration of medicines
3.4 The school will always designate a minimum of two people to be responsible for the administering of medicine to a child
3.5 Staff should never give a non-prescribed medicine to a child unless this is part of an individual Health Care Plan, involving specific written permission from the parents/carers. Where the head teacher agrees to administer a non-prescribed medicine it must be in accordance with this policy. The school will inform parents of this policy. Criteria in the national standards for under 8s day care make it clear that non-prescription medicines should not normally be administered. Where exceptionally a non-prescribed medicine is administered to a child it should be recorded on a form such as Form 5 and the parents/carers informed. If a child suffers from frequent or acute pain the parents/carers should be encouraged to refer the matter to the child’s GP.
3.6 National Guidance states: ‘A child under 16 should never be given aspirin or medicines containing ibuprofen unless prescribed by a doctor.’ The school will inform parents of this policy.
3.7 Any controlled drugs which have been prescribed for a child must be kept in safe custody.
3.8 If a child refuses to take medicine, staff will not force them to do so. Staff should record the incident and follow agreed procedures which should be set out in the child’s Health Care Plan. Parents/carers will be informed of the refusal on the same day. If refusal results in an emergency, the school’s normal emergency procedures will be followed. (Paragraph 49)
3.9 If in doubt about a procedure, staff should not administer the medicine, but check with the parents or a health professional before taking further action.
N.B. The DfE guidance document gives a full description of roles and responsibilities Paragraphs 66 to 102.
4. Parental responsibilities in respect of their child’s medical needs
4.1 It is the parents/carers’ responsibility to provide the head teacher with sufficient written information about their child’s medical needs if treatment or special care is needed.
4.2 Parents/carers are expected to work with the head teacher to reach an agreement on the school’s role in supporting their child’s medical needs, in accordance with the school’s policy.
4.3 The head teacher should have written parental agreement before passing on information about their child’s health to other staff including transport staff. Sharing information is important if staff and parents/carers are to ensure the best care for a child.
4.4 If parents/carers have difficulty understanding or supporting their child’s medical condition themselves, they should be encouraged to contact either the school nurse or the health visitor, as appropriate.
4.5 It is the parents/carers’ responsibility to keep their children at home when they are acutely unwell. Paragraph 83
4.6 It requires only one parent/carer to agree to or request that medicines are administered to a child. It is likely that this will be the parent with whom the school has day-to-day contact.
4.7 Prior written agreement should be obtained from parents/carers for any medicines to be given to a child. (See specimen forms in Appendix A.)
5. Assisting children with long-term or complex medical needs
Where there are long-term medical needs for a child, including administration of medicine for a period of 8 days or more, a Health Care Plan should be completed, using Form 2, involving both parents/carers and relevant health professionals.
5.1 A Health Care Plan clarifies for staff, parents/carers and the child the help that can be provided. It is important for staff to be guided by the school nurse or the child’s GP or paediatrician.
5.2 The school will agree with parents/carers how often they should jointly review the health care plan. It is sensible to do this at least once a year, but much depends on the nature of the child’s particular needs; some would need reviewing more frequently. Paragraph 119
5.3 The school will judge each child’s needs individually as children and young people vary in their ability to cope with poor health or a particular medical condition. Plans will also take into account a pupil’s age and need to take personal responsibility. Paragraph 120
5.4 Developing a Health Care Plan should not be onerous, although each plan will contain different levels of detail according to the needs of the individual child. Paragraph 121
5.5 In addition to input from the school health service, the child’s GP, or other health care professionals, depending on the level of support the child needs, those who may need to contribute to a health care pro forma include:
- The head teacher or head of setting
- The parent or carer
- The child (if appropriate)
- The Early Years Practitioner/Class Teacher
- The care assistant or support staff
- Staff who are trained to administer medicines
- Staff who are trained in emergency procedures Paragraph 122
5.6 The School will consult the DfE publication 'Managing Medicines in Schools and Early Years Settings' when dealing with the needs of children with the following common conditions:
- Asthma
- Epilepsy
- Diabetes
- Anaphylaxis
5.7 Regarding epilepsy, some children may be prescribed rectal diazepam as a treatment for prolonged seizures. Staff involved must have received training from local health services. A written authorisation from the GP, Consultant or Epilepsy Specialist Nurse must have been received for each child, along with instructions for use. Form 9 may be used for this purpose. Two adults must be present for such treatment, at least one being of the same gender as the child. The dignity of the child must be protected as far as possible.
6. Off-site Education
6.1 The school has responsibility for an overall risk assessment of any off-site activity, including issues such as travel to and from the activity and supervision during non-teaching time or breaks and lunch hours.
7. Policy on children carrying and taking their prescribed medicines themselves
An example of this would be a child with asthma using an inhaler.
7.1 It is good practice to support and encourage pupils, who are able, to take responsibility to manage their own medicines. If such medicines are taken under supervision, this should be recorded. Paragraph 45
7.2 There is no set age when a child or young person can take responsibility for their own medication. This needs to be a joint decision between school, parents/carers and the pupil. Please refer to Form 7. Paragraph 46
7.3 Where pupils have been prescribed controlled drugs, these must be kept in safe custody. Pupils could access them for self-medication if it was agreed that this was appropriate. Paragraph 48
8. Staff support and training in dealing with medical needs
8.1 The school will ensure that there are sufficient members of support staff who manage medicines. This will involve participation in appropriate training.
8.2 Any member of staff who agrees to accept responsibility for administering prescribed medicines to a child does so voluntarily and will have appropriate training and guidance. They will also be made aware of possible side effects of the medicines, and what to do if they occur. The type of training necessary will depend on the individual case.
8.3 Teachers’ conditions of employment do not include giving or supervising a pupil taking medicines. Agreement to do so must be voluntary.
8.4 The school will ensure that staff receive proper support and training where necessary, in line with the contractual duty on head teachers to ensure that their staff receive the training. The head teacher, in their capacity as a line manager, will agree when and how such training takes place. The head teacher will make sure that all staff and parents/carers are aware of the policy and procedures for dealing with medical needs. (Paragraph 83)
8.5 Staff who have a child with medical needs in their class or group will be informed about the nature of the condition, and when and where the child may need extra attention.
8.6 The child’s parents/carers and health professionals should provide the information specified above.
8.7 All staff should be aware of the likelihood of an emergency arising and what action to take if one occurs.
8.8 Back up cover should be arranged for when the member of staff responsible is absent or unavailable.
8.9 At different times of the day other staff, such as lunchtime supervisors, may be responsible for children. They will also be provided with relevant information.
9. Record keeping
9.1 Parents/carers should inform the school about the medicines that their child needs to take and provide details of any changes to the prescription or the support required. However staff should make sure that this information is the same as that provided by the prescriber. Any change in prescription should be supported by either new directions on the packaging of medication or by a supporting letter from a medical professional.
9.2 The school will use Form 3A to record short-term administration of medication. Consent forms should be delivered personally by the consenting parent/carer. Staff should check that any details provided by parents, or in particular cases by a paediatrician or specialist nurse, are consistent with the instructions on the container.
9.3 The school will use Form 3B to record long-term administration of medication. Consent forms should be delivered personally by the consenting parent/carer. Staff should check that any details provided by parents, or in particular cases by a paediatrician or specialist nurse, are consistent with the instructions on the container.
9.4 It is the parent/carer’s responsibility to monitor when further supplies of medication are needed in the school.
9.5 Form 4 should be used to confirm with the parents/carers that a member of staff will administer medicine to their child. Paragraph 52
9.6 The school will keep written records of all medicines administered to children, and make sure that parents/carers sign the record book to acknowledge the entry. This is compulsory for Early Years providers; the school has adopted this as good practice for all pupils Paragraph 54
9.7 Although there is no similar legal requirement for schools to keep records of medicines given to pupils, and the staff involved, it is good practice to do so. Records offer protection to staff and proof that they have followed agreed procedures. This school will keep a logbook of medicines given using Forms 5 and 6. Paragraph 55
10. Safe storage of medicines
10.1 The school will only store, supervise and administer medicine that has been prescribed for an individual child.
10.2 Medicines will be stored strictly in accordance with product instructions, in the original container in which the medicine was dispensed, paying particular note to the temperature at which the medicine should be stored.
10.3 Staff will ensure that the supplied container is clearly labelled with the name of the child, the name and dose of the medicine, the method and frequency of administration, the time of administration, any side effects and the expiry date.
10.4 Where a child needs two or more prescribed medicines, each will be in a separate container.
10.5 Non-healthcare staff will never transfer medicines from their original containers. Paragraph 107
10.6 Children will be informed where their own medicines are stored and who holds the key.
10.7 All emergency medicines, such as asthma inhalers and adrenaline pens, will be readily available to children and will not be locked away.
10.8 Schools may allow children to carry their own inhalers. This school will/will not do so. (delete as appropriate)
10.9 Other non-emergency medicines will be kept in a secure place not accessible to children. Paragraph 108
10.10 A few medicines need to be refrigerated. They can be kept in a refrigerator containing food but must be in an airtight container and clearly labelled. There will be restricted access to a refrigerator holding medicines. It is acceptable for a staff room refrigerator to be used for storage, provided that medical items are clearly labelled. Paragraph 109
10.11 Children need to have immediate access to their medicines when required. The school will make special access arrangements for the emergency medicines that it keeps. However, it is also important to make sure that medicines are kept securely and only accessible to those for whom they are prescribed. This will be considered as part of the policy about children carrying their own medicines. Paragraph 111
11. Disposal of Medicines
11.1 Staff should not dispose of medicines. Parents/carers are responsible for ensuring that date-expired medicines are returned to a pharmacy for safe disposal. Return of such medicines to parents should be documented.
11.2 Parents/carers should also collect medicines held at the end of each term. If parents/carers do not collect all medicines, they will be taken to a local pharmacy for safe disposal. This process should be documented. Paragraph 112
11.3 Sharps boxes will always be used for the disposal of needles. Collection and disposal of the boxes will be arranged with the Local Authority. Paragraph 113
12. Hygiene and Infection Control
12.1 All staff should be familiar with normal precautions for avoiding infection and follow basic hygiene procedures
12.2 Staff will have access to protective disposable gloves and will take care when dealing with spillages of blood or other body fluids, and disposing of dressings or equipment.
12.3 Ofsted guidance provides an extensive list of issues that early years providers should consider in making sure settings are hygienic. Paragraph 114
12.4 The Education (School Premises) Regulations 1999 require every school to have a room appropriate and readily available for use for medical or dental examination and treatment and for the caring of sick or injured pupils. It must contain a washbasin and be reasonably near a water closet. It must not be teaching accommodation. If this room is used for other purposes as well as for medical accommodation, the Trustees must consider whether dual use is satisfactory or has unreasonable implications for its main purpose.
13. Access to the School’s emergency procedures
13.1 As part of general risk management processes the school must have arrangements in place for dealing with emergency situations. This could be part of the school’s first aid policy and provision. [See DfE Guidance on First Aid for Schools: a good practice guide, 1998]
13.2 Other children should know what to do in the event of an emergency, such as telling a member of staff.
13.3 All staff should know how to call the emergency services. Guidance on calling an ambulance is provided in Form 1.
13.4 All staff should also know who is responsible for carrying out emergency procedures in the event of need.
13.5 A member of staff will always accompany a child taken to hospital by ambulance, and will stay until the parent arrives.
13.6 Health professionals are responsible for any decisions on medical treatment when parents/carers are not available. Paragraph 115
13.7 Staff should never take children to hospital in their own cars; it is safer to call an ambulance. Paragraph 116
13.8 In remote areas a school might wish to make arrangements with a local health professional for emergency cover. Paragraph 116
13.9 The national standards require Early Years settings to ensure that contingency arrangements are in place to cover such emergencies. Paragraph 116
13.10 Individual Health Care Plans will include instructions on how to manage a child in the event of an emergency, and identify who has this responsibility at different times of the school day.
14. Risk assessment and management procedures
This policy will operate within the context of the school’s Health and Safety Policy.
14.1 The school will ensure that risks to the health of others are properly controlled.
14.2 The school will provide, where necessary, individual risk assessments for pupils or groups with medical needs.
14.3 The school will be aware of the health and safety issues relating to dangerous substances and infection supervisors will need to be very clear regarding their role. Paragraph 117
15. Home to School Transport
The school will ensure that there is effective liaison with drivers and escorts providing home to school transport.
15.1 Prior to transport commencing, transport staff need to be fully briefed about the medical needs of the pupils being transported. Briefing will be given by the school nurse or by another appropriately informed member of staff. In this school, briefing will be carried out by (insert name and designation)
15.2 There should be regular reviews of the situation, in order that that drivers and escorts have up-to-date information
15.3 Where pupils have life-threatening conditions, specific health care plans (or specific essential information from the plan) should be carried on vehicles. The care plans should specify the steps to be taken to support the normal care of the pupil, as well as the appropriate responses to emergency situations.
Appendix for Forms
Form 1: Contacting emergency services
Request for an Ambulance
Dial 999, ask for ambulance and be ready with the following information
1. Telephone number (insert school’s telephone number)
2. Give your location (insert location/address of school and state postcode)
3. Give the exact location in the school of the emergency
4. Give your name
5. Give name of the child and a brief description of the child’s symptoms
6. Give details of any medicines given or prescribed
7. Inform Ambulance Control of the best entrance and state that the crew will be met and taken to the correct location of the school.
Speak clearly and slowly and be ready to repeat information if asked
PUT A COPY OF THIS FORM BY EACH TELEPHONE
Form 2: Health care plan

Form 3A: Parental agreement for school to administer medicine (short term) with head teacher’s agreement and record keeping of administered medication
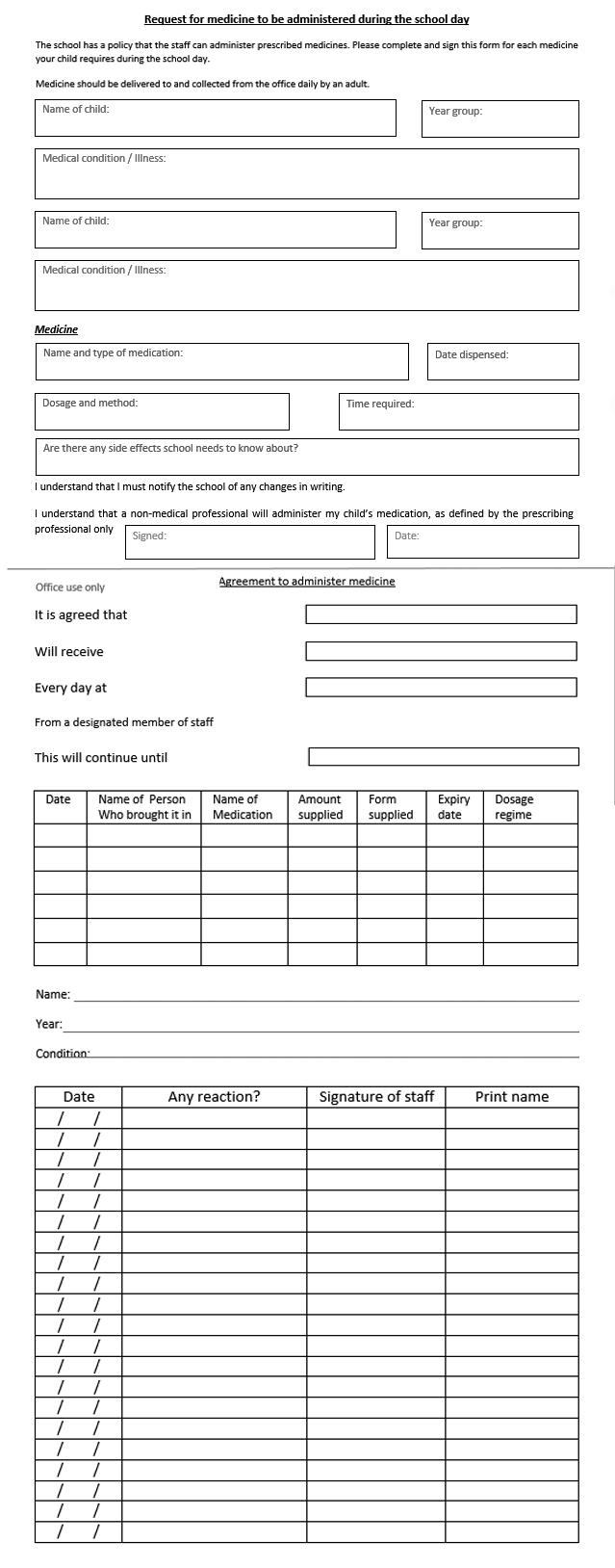
Form 3B: Parental agreement for school to administer medicine (long term) with head teacher’s agreement

Form 4: Head teacher’s agreement to administer medication

Form 5: Record of by whom medication brought into school and when administered

Form 6: Request for child to carry his/her own medication

Form 7: Staff training record

Form 8: Authorisation for the administration of rectal diazepam

Form 9: Authorisation for the administration of Buccal Midazolam

end faq